


COVID-19 Forecast for El Paso County — Nov. 30
Plus, our resident microbiologist on how long immunity from COVID-19 may last
Good morning, and happy Monday. On this pre-pandemic date in 2019, Colorado College’s Women’s Basketball won 64-59 against Macalester College in the final game of the 2019 Rocky Mountain Thanksgiving Classic. (This year, all winter sports have been postponed until January.)
Today, Phoebe Lostroh returns to give her weekly COVID-19 forecast for El Paso County and to explain the hospital capacity in Colorado, a new study suggesting COVID-19 immunity may last years, and the obstacles that one vaccine trial is facing. Lostroh is a professor of molecular biology at Colorado College on scholarly leave who is serving as the program director in Genetic Mechanisms, Molecular and Cellular Biosciences at the National Science Foundation.
➡️ICYMI: On Wednesday, we explained the daily work and protocols of some of Colorado College’s essential workers. We also recapped Colorado’s plan for vaccine distribution.
Phoebe’s Forecasts
NOTES: These forecasts represent her own opinion and not necessarily those of the National Science Foundation or Colorado College. She used the public El Paso County dashboard for all data. Lostroh prepared these forecasts on Nov. 28.
⚖️How her predictions last week shaped up: Nov. 28 was the last day of Morbidity and Mortality Weekly Report week 48 in the national public health calendar. It is the 38th week since the first case was detected in El Paso County. Since March 13, 269 El Paso County residents have died of COVID-19. Last week, Lostroh predicted about 5,544-5,580 new cases of COVID-19 in El Paso County during the week ending Nov. 26. Instead, there were 3,990 new cases.
“The fact that my estimate was too high means that public health interventions begun approximately 3-5 weeks ago are having a positive effect,” Lostroh said.
👩🏻🏫Outbreak Breakdown: According to the El Paso County COVID-19 Dashboard, 23% of local outbreaks — defined as two or more linked cases — have happened at K-12 schools in the last month. That makes schools the single largest category for outbreaks in El Paso County.
Predicted cumulative reported cases in El Paso County
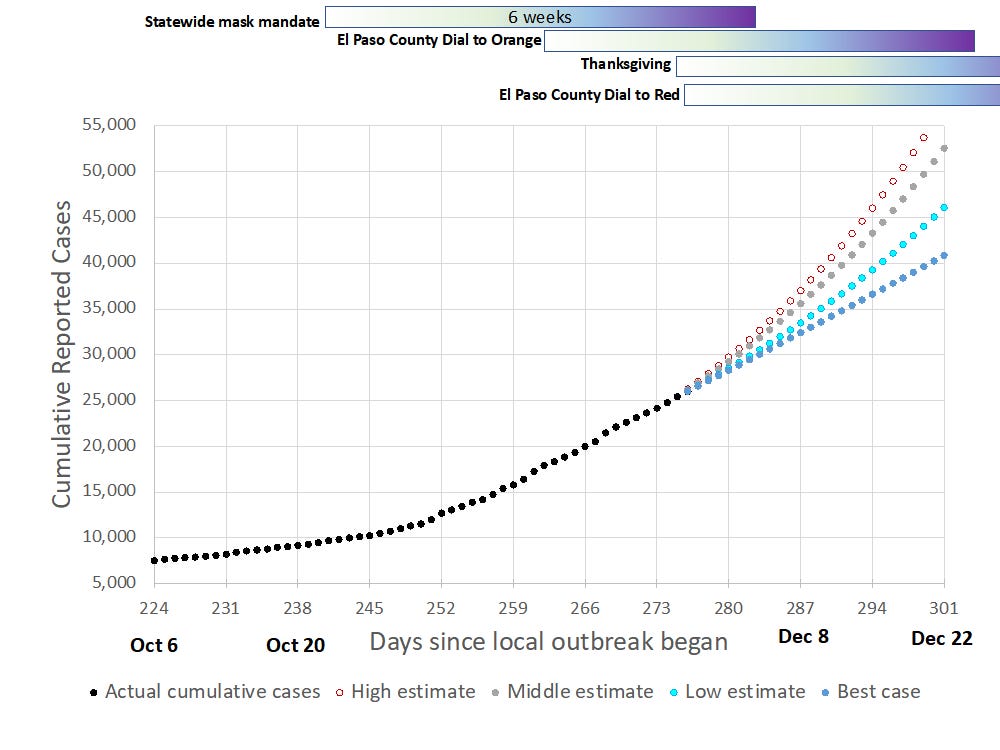
🗝️Key points: The reported cases are represented by black circles. Horizontal boxes filled with a gradient from white to purple indicate the six weeks following an event that affects spread; it usually takes 4-6 weeks for a public-health intervention or a possible spreading event to have an impact on the incidence. Estimates are in red, grey, or blue circles. For the next week, Lostroh predicts El Paso County will see 4,036-4,406 new cases by Dec. 3.
14-day cumulative rolling incidence annotated with changes in local policy and activities

🗝️Key points: The actual calculated incidence is in black Xs, while the other symbols provide estimates based on exponential curve-fitting, or in the best-case scenario, cases remaining almost steady as they have for the last seven days. The thresholds for two of Colorado’s COVID-19 levels are marked with dashed horizontal lines and labeled. Although prevalence crossed into the zone associated with “Level Red: Severe Risk” around Nov. 1, Colorado did not move El Paso County to red-level restrictions until Nov. 27. If that change has a significant impact, Lostroh predicts the county will probably see incidence close to, or even below, the best-case prediction.
“The good news means that we are flattening the curve, but it also leaves us in the red zone until at least Christmas,” Lostroh said.
14-day rolling incidence and 14-day rolling percent positivity in Front Range counties

🗝️Key points: Data is from the Colorado COVID-19 Dial Dashboard. Incidence in Pueblo is about six times higher than the “Level Red: Severe Risk” threshold of 350, while Denver, El Paso, Adams, and Weld counties are 3-4 times higher than the threshold. Effective contact tracing needs a test positivity rate of less than 5%, which none of the depicted counties have.
Cumulative reported hospitalizations and deaths from COVID-19 in El Paso County

🗝️Key points: Hospitalizations are plotted on the right-hand axis using red, while deaths are plotted on the left-hand axis using black. By using two axes, you will be able to see the shape of each curve more clearly. The last two weeks have a hospitalization rate of around 3.1% and a case fatality rate of around 0.55%, which Lostroh calculated using the total number of reported cases in those two weeks as the denominator.
Q-and-A with Lostroh: Our resident microbiologist on Colorado’s hospital capacity
This interview has been edited for length and clarity.
CC COVID-19 Reporting Project: What can you tell us about hospitals across the country nearing capacity because of rising COVID-19 cases? How do hospitalization rates look in Colorado?
Lostroh: I think that we probably are going to run out of people before we run out of PPE in Colorado. What’s happening now is that the healthcare workforce is getting sick because the disease is so common in our community. We already have a shortage of nurses. What happens if some nurses at a hospital get sick and catch COVID? Not even necessarily at work, but in the community, because they’re at the grocery store. They’re taking every precaution, but when you’re taking every precaution and the incidence is very high, somebody’s going to get sick anyway. Now, Colorado’s statewide COVID dashboard has a metric called ‘decreasing or stable hospitalizations.’ Counties that have had declining or stable hospitalizations for 12-14 days are colored green; counties with zero to seven days of declining or stable hospitalizations are colored red. That metric on the dashboard doesn’t match what’s happening in the press. So for instance, there were stories last week about how Weld County only had three ICU beds left, and yet their county was still green on the dashboard at the time. (Editors’ note: It has since changed to yellow). Here in El Paso County, it says ‘five days of declining or stable new hospital admissions.’ But when you look at the hospitalization data, that doesn’t match the words. We are not getting accurate information about hospitalizations in Colorado or in El Paso County. That worries me. ... On the other hand, our numbers have leveled out, so I’m really excited about that. It happens to be four weeks from when the governor said to stop gathering in small groups outside your own household and to wear a mask everywhere indoors. So I think that’s really good — the flattening of the incidence curve is a really good sign. We have to get it flat before we can reverse it; I’m just not sure if we’ve really reversed it yet. Of course, we’ve flattened it under a situation where the hospitals are already almost full in some places, so it would have been better to have flattened it several weeks ago.
CCRP: Recently, the New York Times reported a new study found that immunity to the coronavirus may last for years. To what extent might immunity to COVID be long-term, as opposed to the three-month immunity period that some people previously predicted?
Lostroh: I think there was circumstantial evidence from the beginning that lifelong or long-term immunity would be difficult to achieve with COVID-19 because it had never been observed to happen in other coronaviruses before. The coronaviruses with which we have the most experience cause mild infections, and people get them over and over again over their lifetimes. The reason that we all thought that immunity might be short-term, even though we were hoping it wouldn’t be, is mainly because of our experience with these other human coronaviruses. Then we have reports coming in from places like China, where they started taking antibodies from people and tracking the levels of antibodies in their blood over time. What they found was some people made a high amount of antibodies for a long period of time, and some people made a low amount of antibodies for a short period of time. There was somewhat of a correlation between the severity of the infection and whether they got high or low antibodies that lasted for a longer or shorter amount of time. We know that for a lot of other infections, the amount of antibodies in your blood is a good correlation for whether or not you remain protected from that infection. It’s unusual to have good lifelong or long-term immunity without having antibodies. … Now that said, instead of antibodies, you can study the cells that are responsible for remembering an exposure to a harsh pathogen and for springing into action to make antibodies and to make killer T cells and helper T cells in response to the second exposure to a pathogen. … If you study that, you can find that people do have memory immune cells that will probably provide protection to some people for longer than there are antibodies easily detectable in their bloodstream. So I think the evidence is still mixed.
CCRP: To your understanding, why did some scientists raise doubts about the conduct of AstraZeneca’s clinical trials for their COVID-19 vaccine last week, potentially setting back its authorization for use in the U.S. and Europe?
Lostroh: I’m not surprised that AstraZeneca ran into problems. What I am surprised about is that companies like Pfizer-BioNTech and Moderna have not run into problems. ... I think with AstraZeneca, they were worried the vaccine only had 60 or 70% efficacy, and then also the weird thing was that the low dose seemed to provoke a stronger immune response than the higher dose. That is weird and requires further investigation in terms of the dose response being the opposite of what you typically see with a vaccine trial. But only being 60 or 70% efficacious in terms of preventing disease, that’s pretty normal. So for instance, influenza vaccines provide sometimes even less protection than that, but that’s not an unusable vaccine. The issue with vaccines is we give them to healthy people. And since we give them to healthy people, the ethical standard of how much risk we can tolerate is much higher than for a pharmaceutical or other treatment given to somebody who is already ill. If you can make somebody sick who is well, that’s a different set of ethical considerations for any kind of intervention. So for a vaccine to be worth the risk of administration, you would like to see much higher efficacy than 60 or 70%. Now in the case of influenza, influenza is actually a very deadly disease, so we tolerate only 50 or 60% protection because of how deadly it otherwise is, and because even that level provides a lot of protection to the whole population.
About the CC COVID-19 Reporting Project
The CC COVID-19 Reporting Project is created by Colorado College student journalists Miriam Brown, Isabel Hicks, and Esteban Candelaria in partnership with The Catalyst, Colorado College’s student newspaper. Work by Phoebe Lostroh, Associate Professor of Molecular Biology at CC and National Science Foundation Program Director in Genetic Mechanisms, Molecular and Cellular Biosciences, will appear from time to time, as will infographics by Colorado College students Rana Abdu, Aleesa Chua, Sara Dixon, Jia Mei, and Lindsey Smith.
The project seeks to provide frequent updates about CC and other higher education institutions during the pandemic by providing original reporting, analysis, interviews with campus leaders, and context about what state and national headlines mean for the CC community.
📬 Enter your email address to subscribe and get the newsletter in your inbox each time it comes out. You can reach us with questions, feedback, or news tips by emailing ccreportingproject@gmail.com.